As an expert in periodontology at Vélez y Lozano, you can imagine that many times a month I explain to a patient what is wrong with him/her and how I know, because there are many questions that arise in this regard. That is to say, when I tell a person sitting on the couch that they must undergo a certain treatment and that they must go for check-ups every so often, they almost always ask: And on what criteria do you base your decision?
It is true that not all patients who suffer from the periodontal disease are at the same point, and of course there are predefined criteria in the clinic that allow us to distinguish between one or the other protocols to be applied depending on the case we are dealing with.
But, and although I sometimes feel I am repeating myself, before going into this subject we have to go back a bit, because otherwise the patient cannot understand it.
What is periodontitis?
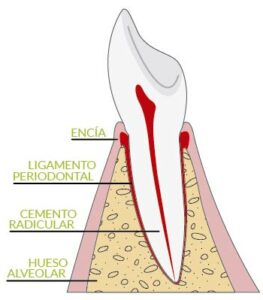
Periodontitis is the most advanced stage of periodontal disease and is characterised by the destruction of the supporting tissues of the teeth, such as the gum, root cementum, periodontal ligament and bone.
One of the main problems with this disease is that it can go unnoticed for many years, because it is not always accompanied by symptoms, and does not produce visible aesthetic changes in its early stages.
This is why we insist on the importance of early diagnosis, which prevents irreversible consequences (gaps between teeth, dental mobility, loss of teeth, etc.).
And here comes the issue at hand,
How is a periodontal patient diagnosed (and classified)?
Well, to diagnose the disease we use different tests:
- Oral examinationThe first test, with a more limited scope, is the first oral examination that takes place in the office, with the patient in the dental chair. Obviously, as we have already explained, periodontal disease is sometimes asymptomatic and does not produce noticeable aesthetic changes in its early stages, so this type of examination has its limitations. However, we will examine the patient in search of warning signs such as the appearance of the gums, the colour or shape of the gums, any signs of inflammation, tartar build-up in the area, bleeding, etc.
- X-raysRadiological tests are obviously a more reliable and concise way of detecting this and other diseases. In the case in question, they allow us to discover whether there has been loss in the insertion area of the tooth, which as we have already seen is a typical characteristic of periodontitis. In addition, these tests allow us to locate the most affected areas and quantify bone loss.
- Periodontogram: This is, without a doubt, the key test, which is carried out by means of different probes that allow us to locate the periodontal pockets and analyse their depth and size. I will explain it in more detail:
What is a periodontogram?
The periodontogram is a kind of 'gum map' in which we capture a series of data about the health of the patient's gums in a graph in order to make a diagnosis with as much information as possible. When it is carried out, we already know that the patient is a periodontal patient, and the objective is to be able to plan a quality treatment to solve the patient's current problem.
The periodontogram is performed by means of probing, which gives us direct access to the innermost part of the periodontium, providing us with clear and precise information about the presence of periodontal pockets, the site of this infectious problem.
This allows us to draw this 'gum map', noting where these periodontal pockets are located, their size and the depth at which they are located. The aim is to make an effective diagnosis, in order to subsequently design a personalised periodontal treatment.
How is a periodontal patient classified (and treated)?
"So... how do you classify and decide the treatment of a periodontal patient," you may be asking. Although it is not an exact science, we can say that periodontal pockets between 1 and 3 mm (calculated with the probing I explained before) are usually associated with a healthy pocket. Those of 4 mm already show signs of mild or moderate periodontitis and those larger than 5 mm can no longer be adequately cleaned and require other types of treatment.
Therefore, and listing, according to the results of the tests described above, we can speak of patients with:
Gingivitis: Inflammation and bleeding gums occur, but periodontal probing is not necessary and no bone loss has occurred. It will be treated with dental prophylaxis and instructions in patient-specific hygiene techniques.
Mild and/or moderate periodontitisWhen there is already bone loss and probing of more than 3mm, in addition to abundant plaque and tartar accumulation, a 'deeper' prophylaxis is necessary. This treatment is known as scaling and root planing or curettage and is based on cleaning the teeth below the gum under local anaesthesia. It is usually performed in several sessions and also involves the use of antibiotics and specific antiseptics.
Advanced periodontitisIn cases in which the bone loss is very high and the anchorage of the teeth has diminished notably (in this phase we usually find mobility in several teeth) it is usually necessary to perform gum surgery, extract the most affected teeth and replace them with dental implants.
I hope this has cleared up some of your doubts, although I will always be available to assist you, both in networks and in the comments section and, of course, in the office.